On April 18, 2026, the ACOG published updated guidance on evaluation of postmenopausal bleeding. This directive fundamentally changes how clinicians must approach a symptom experienced by roughly ninety percent of patients ultimately diagnosed with uterine cancer. The medical landscape shifted significantly this week. A crucial mandate from Washington has officially ended the era of passive observation in women's healthcare.
It is a swift and necessary departure from isolated imaging protocols.
Dr. Steven J. Fleischman, the ACOG President, explicitly detailed the necessity of this operational update. Endometrial cancer incidence in the United States has climbed steadily for several decades. The historical reliance on ultrasound alone as a triage tool is no longer clinically sufficient. The revised framework is designed to prioritize prompt diagnosis above all else.
The clinical margin for diagnostic error is simply too high to ignore.

Dr. David Shalowitz, a gynecologic oncologist and the author of the guidance, noted a meaningful shift in methodology. He stated that using endometrial thickness by ultrasonography yields an unacceptably low sensitivity for malignant pathology.
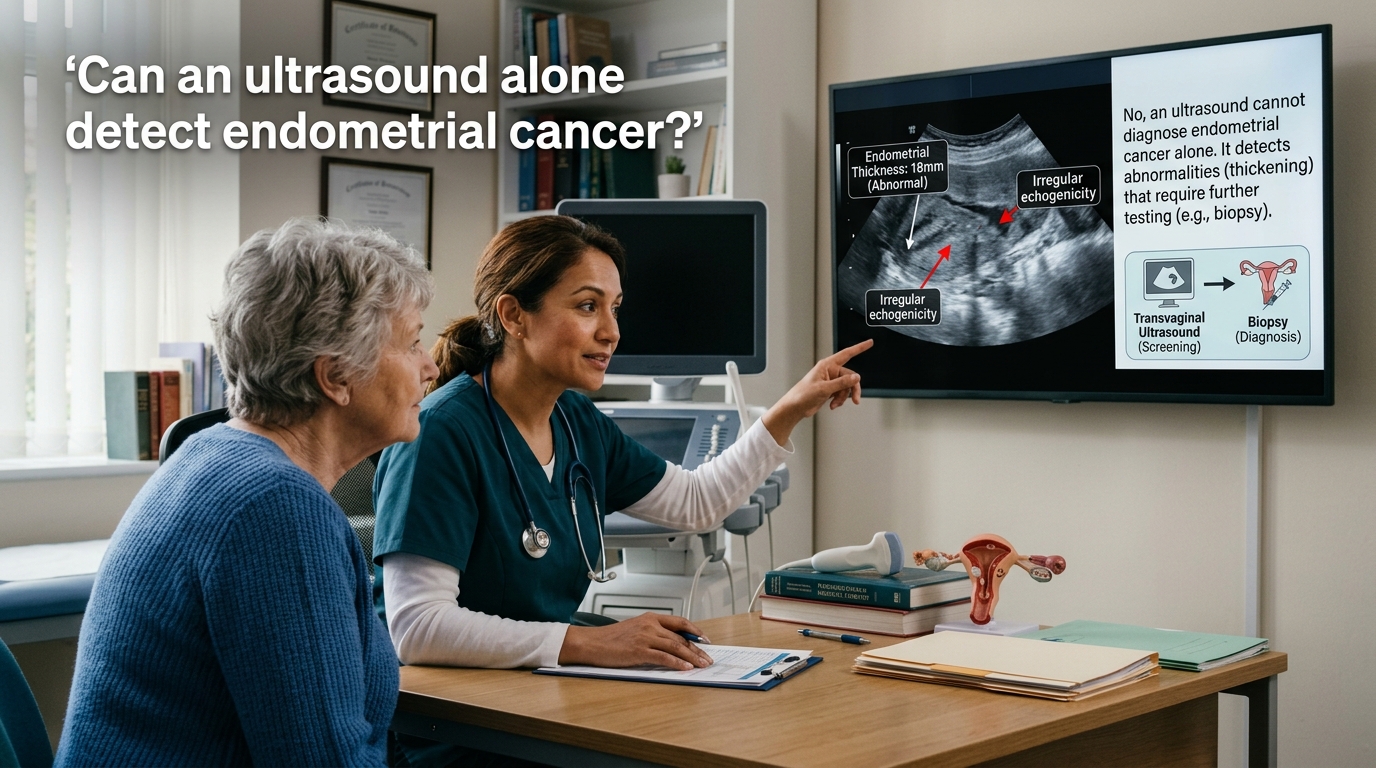
Recent statistical data underscores this glaring vulnerability in women's healthcare. Studies suggest that between five and twelve percent of cancers evade diagnosis upon initial presentation when practitioners rely solely on ultrasonography. The updated clinical practice framework directly addresses this gap by mandating a combination of transvaginal imaging and immediate tissue sampling.
The primary goal is to eliminate the false reassurance of a clear scan.
This dual diagnostic requirement actively reduces the risk of a missed malignancy. It serves as a focused update to related content in Committee Opinion 734. The previous standards allowed for a more passive approach to early screening. Now, the baseline expectation involves securing physical tissue samples from the endometrium during the very first clinical evaluation.
The guidance also addresses a deep and persistent inequity in healthcare outcomes. The update highlights the disproportionate incidence and mortality rates of endometrial cancer among Black women.
Comprehensive screening is vitally important for this specific demographic.

By recommending tissue sampling as a baseline for most patients, ACOG creates a definitive pathway to detect and treat premalignant conditions early. The guidance acknowledges that patients are far more likely to undergo endometrial sampling when provided with patient-centered counseling. Clinicians are urged to share comprehensive educational materials before any procedures.
Educational transparency plays a crucial role in mitigating the anxiety associated with biopsies. The decision to proceed with endometrial sampling must result from shared decision making. It must always reflect the core values and preferences of the patient.
This combined approach may also reduce healthcare burdens across the board. Patients who have limited access to prompt radiologic and oncologic care benefit immensely from a single comprehensive initial evaluation. It fundamentally limits the need for multiple stressful return visits.
Efficiency in clinical diagnosis directly translates to better survival rates.
The private sector market is already responding to this urgent diagnostic shift. Companies like PinkDx are actively developing non-invasive testing alternatives to complement the new standards. Following a massive initial funding round, the company recently highlighted their focus on a simple vaginal swab designed to detect molecular signals associated with endometrial cancer.
Innovation is aligning perfectly with strict clinical mandates.
As professional medical bodies refine their care pathways, the demand for sophisticated diagnostic tools will inevitably surge. A combination of rigorous guidelines and private sector innovation is currently reshaping gynecologic oncology.
The medical community can no longer afford to be passive regarding postmenopausal bleeding. The bleeding is defined as occurring twelve or more months after the final menstrual period. The era of diagnostic ambiguity is officially coming to a close. This updated guidance provides a robust and uncompromising framework that prioritizes the immediate health of women.
Frequently Asked Questions
What is considered postmenopausal bleeding?
It is defined as bleeding presumed to be from the uterus twelve or more months after a patient's final menstrual period. It is a critical symptom that requires immediate medical evaluation.
Why did ACOG update its diagnostic guidance?
The incidence of endometrial cancer has been rising steadily for decades. ACOG determined that relying on ultrasound alone missed a significant number of cancer diagnoses during initial clinical presentations.
What are the new recommended tests for postmenopausal bleeding?
The updated guidance recommends a combination of transvaginal ultrasonography and endometrial tissue sampling. This dual approach is now the standard for the initial evaluation of most patients.
Can an ultrasound alone detect endometrial cancer?
Not with absolute certainty. Recent data indicates that five to twelve percent of cancers may not be diagnosed if clinicians rely exclusively on ultrasound imaging without a physical tissue biopsy.
How does this clinical update impact Black women?
The update explicitly addresses the disproportionate incidence and mortality rates of endometrial cancer among Black women. It emphasizes that a combined diagnostic approach is particularly critical to improving outcomes for this population.
What is Committee Opinion 734?
It is a previous clinical document that outlined the role of transvaginal ultrasonography in evaluating postmenopausal bleeding. The new ACOG mandate serves as a highly focused update to this older framework.